Sacroiliac dysfunction and Lumbo-pelvic dysfunction
Lumbo-Pelvic and Sacroiliac Joint Dysfunction Treatment in London
Sacroiliac joint dysfunction is a common yet often overlooked cause of pain in the lower back, hips, and legs. The sacroiliac (SI) joints play a crucial role in the function of the lumbo-pelvic area, serving as a foundation for the spine. These joints connect the sacrum (the base of the spine) with the iliac bones of the pelvis, forming the pelvic girdle. The SI joints act as shock absorbers, transferring forces between the lower body and the trunk, allowing for movement and flexibility.
When there are restrictions or dysfunction in the sacroiliac joints, the effects are often felt in other parts of the body too, such as the lower limbs or spine, before becoming apparent as a direct issue with the joint itself. While imaging such as X-rays or MRIs can detect large changes in the sacroiliac joints, they often fail to identify subtle restrictions that can lead to pain and dysfunction. These minor restrictions, though invisible in scans, can have a significant impact on mobility, muscle coordination, and overall joint stability.
Why Sacroiliac Joint Dysfunction is Crucial to Treat
Sacroiliac joint dysfunction can lead to a cascade of issues in the body, particularly affecting the lower back and lower limbs. It is nearly impossible to find a spine pathology or lower limb issue without some degree of dysfunction or restriction in the SI joints. Therefore, treating the sacroiliac joints is often the first step in effectively addressing and resolving related pain or dysfunction.
By normalizing the movement of the sacroiliac joints and the surrounding connective fascial tissues, treatment can enhance coordination, improve muscle recruitment, and increase range of motion. This, in turn, leads to pain reduction, enhanced stability, and a more natural sense of movement. This normalisation happens with targeted manual therapy and exercise therapy techniques.
Common Conditions Treated by Sacroiliac Joint Normalization
Effective treatment of the sacroiliac joints can lead to significant improvements or complete resolution of symptoms associated with various musculoskeletal and pelvic conditions, including:
Piriformis syndrome
Sciatica
Bulging and herniated discs
Facet joint syndrome
Spondylolisthesis
Trochanteric bursitis
Gluteal tendinopathies
Hip osteoarthritis (OA)
Pelvic floor dysfunction, including incontinence
Pudendal nerve compression
Endometriosis-related pelvic pain
Patellofemoral tracking issues
Chondromalacia patella
Meniscus issues
In cases of these conditions, addressing sacroiliac joint dysfunction can have a profound impact on reducing pain and restoring function, particularly in cases of chronic pain that affect posture, movement, and quality of life.
How Sacroiliac Joint Treatment Works
The treatment for sacroiliac joint dysfunction typically involves soft tissue techniques and gentle mobilization to encourage normal movement within the joint and surrounding fascia. One commonly used technique is osteoarticular pumping, a semi-active treatment, where the therapist guides the patient through gentle muscle contractions to help influence the opening and closing of the SI joints. This movement promotes the flow of synovial fluid and stimulates the ligaments, helping reset the resting tension and proprioceptive function of the ligaments.
Patients generally experience the treatment as pleasant, with a sense of relief and relaxation. The gentle, non-invasive techniques aim to restore fluid movement and alleviate discomfort, making it an excellent option for individuals seeking natural, effective pain relief for lower back, pelvic, and hip pain.
Patients will be taught specific exercise techniques, such as myofascial stretching, segmental muscular strengthening and ELDOA™ exercises specifically for the sacroiliac joint. This is crucial in order to maintain and continue to improve the effects of the treatment.
Peter offers a range of treatments for sacroiliac (SI) joint pain and lumbar-pelvis issues in London, focusing on a holistic approach that addresses both physical and emotional aspects of pain. The therapies employed aim to alleviate discomfort, restore function, and promote overall well-being. This approach respects the complexity of the human body and the interconnectedness of its systems.
The Sacroiliac Joint Explained
The sacroiliac joint once was thought to be a joint that had no significant movement and function. I recall occasions in our multidisciplinary meetings just a few years back where even reputable doctors and radiologist have doubted this joint's significance.
Even though there have been multiple studies detailing the anatomy of these joints it is relatively safe to say that its mechanics are still poorly understood and questioned as it is hard to accurately quantify its range in a living subject.

Andrew Vleeming examined the different shapes and auricular surface orientation of many different cadavers and found a huge deviation between them. Not only the width and length of the auricular surfaces of the greater and lesser arms were considerably different, their orientation relative to the horizontal and vertical planes varied. Sometimes the lesser/short arm was greater than the greater/long arm of the joint, sometimes it was the other is compared to the shape of a letter L was consistent and even though there were differences between their orientation relative to horizontal and vertical planes the deviations were consistent.
Given the logical assumption that primarily joint surface shape and orientation determine the available movement within the joint (arthro-kinematics) with a secondary check from the capsule and ligamentous apparatus surrounding it, the question is not whether there is a significant enough movement that exists in these joints but in what direction and to what degrees. This is something that seems to be very hard to accurately quantify. I believe that the knowledge of relational anatomy of the pelvis is essential in understanding, palpating and interpreting what the hand is picking up of the SIJ's small but impactful movement.
To date, I haven't come across a better explanation, with such logical anatomical and biomechacanical reasoning of how the sacroiliac joint moves, correlating it to everyday clinical presentations than the one in Guy Voyer DO's teaching. In fact, I have witnessed hundreds of patients being treated by him based on his mechanical understanding of the sacroiliac joint and the results were exceptional. Many of these people had previously exhausted all other rehabilitation methods and medical treatments, including surgery with limited success. But their body changed, often immediately when treated based on this understanding. Seeing this made me decide to start doing Voyer's osteopathic training.
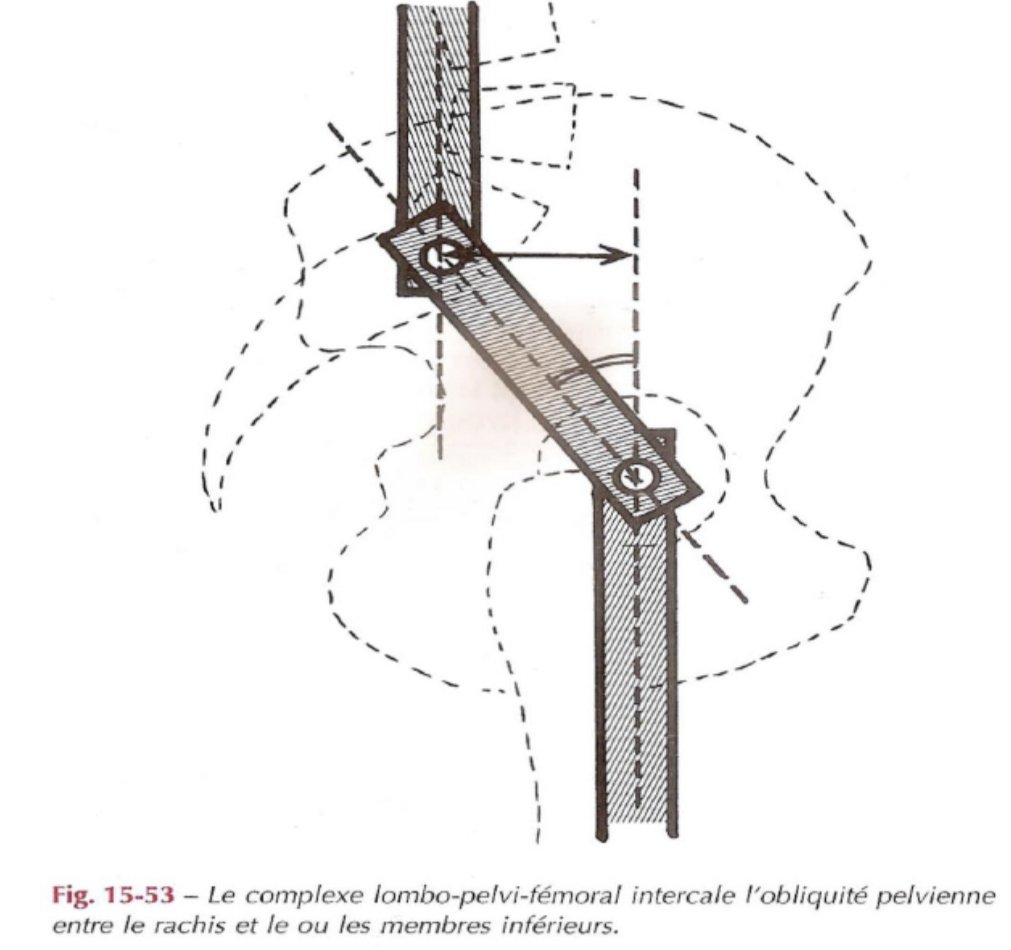
The sacroliliac joint functions as a connecting rod a sort of "shock absorber" that transfers the ascending ground forces through the movement of the lower limbs to the trunk and the descending forces generated by the trunk and the upper limbs to the lower limbs.

These forces are not aligned in any way. From a sagital view the descending forces coming via the sacrum are posterior the ascending forces coming from the femoral head. In frontal plane view they are medial to the descending forces.

The SIJ and its ligamentous apparatus absorbs and transfers those forces from lower to upper body and vice versa.

The bony trabeculae are thin columns, the internal reinforcement of the bone that builds up in relation to the pressure and tension imposed on the bone. These internal pillars are continous and can be seen as a representation of line of force transmission inside the bones as well as bone to bone. Collagen fibre orientation inside joint capsules and ligaments often look in line with Trabecular alignment coming from the sacral vertebrae and continues in different lines towards the ischial tuberosity, pubic branch and the coxa-femoral joint from where it continues to the femoral head, neck and the shaft etc.
The SIJ is a transfer of these forces and the line of tension represented by the bony trabeculae forms in different joint position in relation to the ilium, ischium and pubis. If joint alignment is disrupted, trabecular continuity will be disrupted too, which asks for remodelling in relation to the changed loading. We know the importance of trabecular alignment in the case of joint wear and tear and osteoarthritis. In order to have a basic understanding of SIJ mechanics we need to have a quick look at the anatomy surrounding the joint.
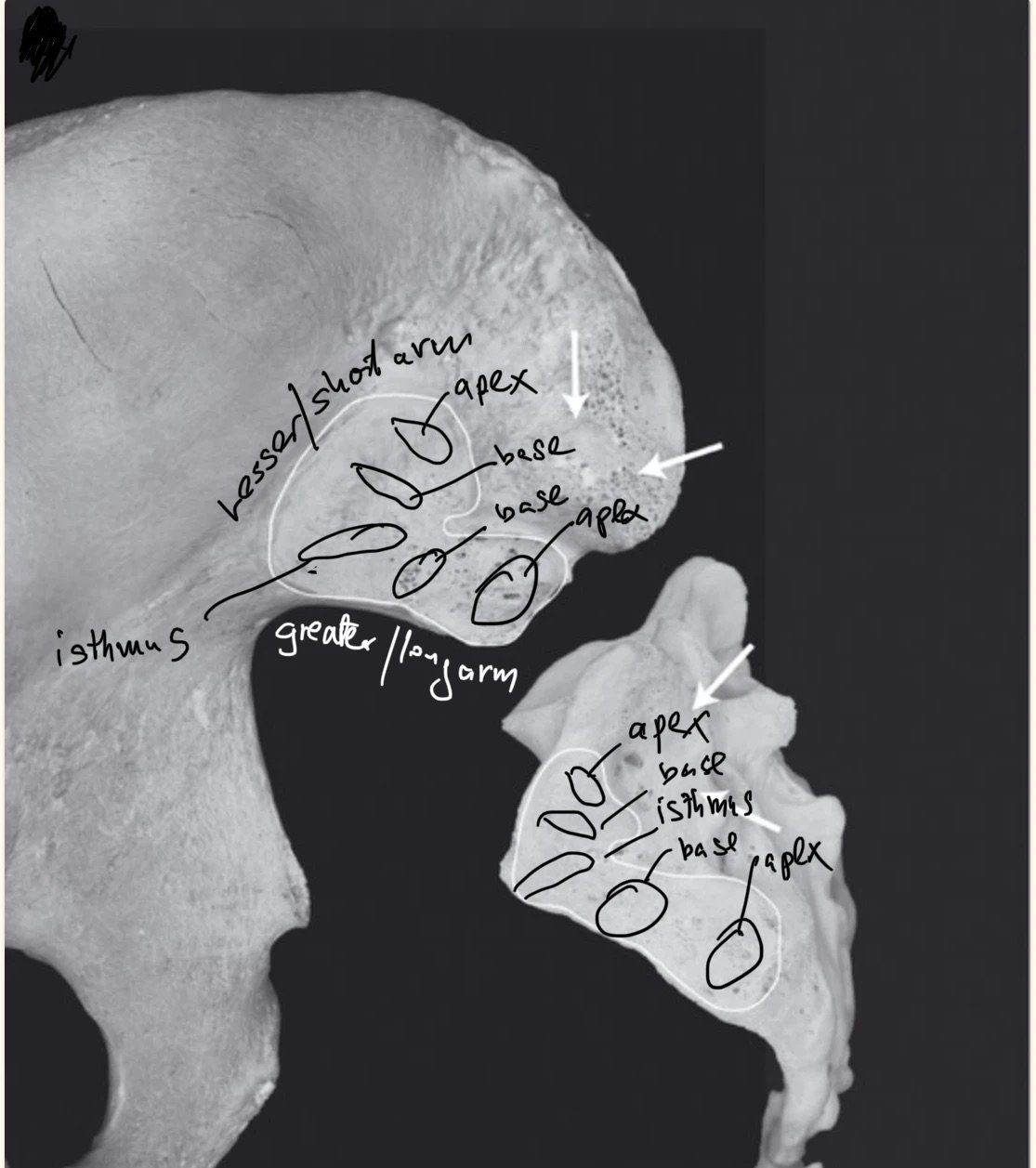
The auricular surfaces
The joint surfaces that articulates with one another are called the auricular surfaces. The short arm or lesser arm runs antero-inferiorly and its orientation is closer to the vertical plane. The long arm or greater arm of the SIJ is running antero-superiorly and its orientation lies closer to the horizontal plane. The two arms meet at the isthmus forming a shape resembling a letter "L". The end/tip of each arms are called the apexes, while the root of each arms called the bases. The isthmus is the most anterior part of the joint where the two arms meet.

Basic review of the Axis of the Pelvis & SIJ
It is important to note that I'm not saying that these are the only movements possible. What I'm saying is that based on Guy Voyer DO's 40+ years of clinical practice and vast experience these are the movements that have proven to be the most accurate representation of the how these joints may function.
The 22 virtual axes of the pelvis can be divided into 5 groups:
3 horizontal axes
2 oblique axes
9 AP axes
5 vertical axes
3 axes of the pubic symphysis
While this sounds a bit of a mouthful, it is important to understand that many of the above axes only occur as compensatory movement mechanism as a result of restriction due to, muscles spasm, osteophytes, arthritis, cysts, visceral lesion just to name a few, therefore they are pathologic. The body's goal is to always complete an oblique axes and the pathological axes are compensations of the body trying to move normally with the given restriction. These pathological axes are in line with or are assigned to the various landmarks of the joint and are 'acted out' as compensatory mechanism in the body's attempt to continue to move in the path of least resistance.

The horizontal (H) axes run in the frontal plane.
H1 is at the level of the first sacral vertebra and it is Sutherland's cranio-sacral movement - (sacrum-occipital)
H2 is the movement of counter-nutation and nutation as the superior and inferior pelvic outlet opens during delivery.
H3 is the movement of the ilium in posteriorization, anteriorization, inflare and outflare relative to the sacrum and it is called iliosacral movement.
Anteriorization and posteriorization are both movements of the ilium in the sagital plane. Inflare and outflare are similar movements of the ilium with an additional component of flaring - which results in a slight frontal plane deviation where the ASIS moves medially with outflare, and the PSIS moving medially with the inflare.
The terminology of inflare and outflare may be taught slightly differently in other schools of thoughts so it's worth keeping it in mind.
These are physiological movements that happen in conjunction with the sacrum's movement on its oblique axes.

The oblique axes
These axes run from the apexes of the lesser arm to the controlateral apex of the greater arm. This is a sacroiliac movement or the movement of the sacrum relative to the ilium. The sacrum performs the movement of positive torsion (flexion+rotation) and negative torsion (extension+rotation).
During gate the sacrum moves from positive to negative torsion and the ilia move between inflare and outflare.
These are physiological or healthy movements of the pelvis.
Now imagine you had a harder than usual workout where you loaded a bit heavier than you should have. You happen to be on the more mobile end of the mobility scale and the next day one side of your lower back feels very stiff. This stiffness comes from a small spasm of your right iliocostalis lumborum which when retracted can directly impact the full range of the movement of the ilium into inflare, just as a tight biceps would limit the degree you could fully straighten your elbow.
This has a knock on effect of the surface area the femoral head engages the acetabulum, therefore, the ligaments of the hip joint, the rotation range of the femor, therefore the knee and so on going down the chain. Not to mention the anterior ilium will create a false long leg on the side as the femor is pushed inferiorly with a component of relative internal rotation. The sacrum will side-bend and the lumbar spine will have to adopt and so goes up the chain to the thoracic spine, scapulae and cervical spine.
Our muskuloskeletal system serves as a container in which our visceral system exists. Lot of the organs are literally suspended between these bony levers and when the position of these bones change, the tension of these suspensory ligaments of these organs can create a tension, torsion or create a position that results in compression which can result in altered function overtime. Just think of the lumbo-ovarian ligament, the utero-sacral ligement or pubo-vescical ligament where the ovaries, uterus and bladder rely on an ideally symmetrical pelvis. This is one very simple example that's meant to remind us to the importance of looking at relational anatomy and its functional physiological correlations.
What isn't normal
Pathological axes develop as a result of trauma, micro-trauma or prolonged imbalances mainly on the apexes and bases of the lesser and greater arms as part of the compensatory mechanism of the body trying to move normally. The sacrum wants to complete its positive and negative torsion and the ilia want to move into inflare and outflare.
The following axes are non-physiological, where normal torsional movement of the sacrum is not possible that results in an abnormal movement as a compensation.
Antero-posterior (AP) axes - a restriction of mobility on either the apexes or bases of either the lesser or the greater arms and there is a central AP axe that goes directly in the middle of the sacrum = 9 AP axes
Meaning the sacrum wants to do a positive torsion (flexion+rotation) or negative torsion (extension+rotation) on the oblique axe but there is a restriction of mobility on the base of the greater arm (this creates an axe that will disturb the normal torsional movement of the sacrum and will likely to result in an additional abnormal side-bending of the sacrum.
Vertical Axes - these are restriction of mobility at the end of the range in the apexes of either the lesser or greater arms with one central axes - 5 Vertical axes These lesions are very painful and often results in "spraining" the posterior sacroiliac ligamentous complex and/or the pubic synthesis.

The axes of the pubic symphysis
While there is movement at the symphyses pubis, in reality these axes don't exist. They are lesions on planes of movement, in which there is a mixing of axes as a consequence of one of the above lesions (vertical etc.) resulting in torsion, compression or separation of the symphyses pubis.
These are movements of necessity as a result of compensation.
1. Sagital plane: superior and inferior movement of the pubis symphysis.
2. Horitonal plane: anterior and posterior movement of the pubis symphysis.
3. Frontal plane: There is a torsional component to the movement through the meniscus and interosseous ligaments.
There are also other "lesional" axes such as nutcracker lesions (total, hemi, hemi cephalic or caudal, reverse nutcracker etc.) when the joint is partially "off track"of the joint surface.
The above are just a brief explanation of some of the possible pathological movements of these joints. These lesions can happen simultaneously where the combination of two exists as the body's compensation will create a secondary lesion.
In my experience it is very hard to find someone suffering from virtually any type of back, hip, knee or foot and ankle problem with a perfectly aligned sacroiliac joint. Many of these cases where the SIJ is corrected the pain itself will reduce in intensity and in some cases disappears completely.
Lumbo-Pelvic and Sacroiliac Joint Dysfunction Treatment in London
SomaTherapy in London treats pelvic, sacroiliac joint and pelvic floor dysfunction with specific manual therapy techniques that normalise each part of the joint and its biomechanically significant ligamentous, fascial and muscular links. Treatment comes hand in hand with exercise therapy where very specific exercises are given at the end of the session to target the very tissue that's been treated.
These SomaTraining exercises act as a mini treatment, a type of self administered version of the treatment in micro-dosing that you can do yourself at home. These techniques are very powerful and give the steering wheel back into your hands where you gain control back over your health.