Post-Covid Myocarditis and Pericarditis
Having treated one of my long term client for post covid myocarditis with good symptomatic relief, her GP started referring me patients who suffered the same problem.
Myocarditis and pericarditis are conditions when either the muscle or the sac of the heart inflames. In some cases both. These conditions can severely affect the heart's ability to fulfil its normal function resulting in heart palpitations, tightness around the chest and the rib cage, sharp stabbing pain in the heart, often accompanied by shortness of breath and fatigue with many unable to carry on their normal daily activities and work.
According to NHS data up to 10 per cent of COVID-19 patients in the UK suffer from ‘long COVID’ and it is thought that many patients who have had COVID-19 have ongoing inflammation in their heart. Many people aren't really aware and put some of these symptoms down to other things and continue to push themselves through their days.
Two of my now serious long COVID heart patients both recovered from COVID-19 infections, then a week or two later they started to resume their daily routines and exercise schedules and even though they felt a bit sluggish they just pushed through it. 2-3 weeks after that they both crashed with fatigue. and struggled to function normally. Wondering what's going on with a roller coaster of symptoms they struggled to function normally then diagnosis came. As a precaution I'd advice people to be very gradual with resuming their activities after a Covid infection as chances are there is a minor underlying inflammation which can be triggered by exertion.
If you are a fit person who's used to train hard and have inflammation of the heart without much symptoms during your daily activities and you decide to go out and train hard, say do a HIIT class or go sprinting, that could turn out quite bad for you so it's better to be on the safe side and be gradual.
I had suggested to several clients over the past couple of years to go to get their heart checked when their symptoms seemed like it could be a heart problem. Unfortunately a few did turn out to have a mild myocarditis almost all those people did have something on their heart that caused hearts checked when I was suspicious of their symptoms which they simply put it down to long-Covid fatigue but in reality the fatigue turned out to be a symptoms of heart muscle inflammation.
In my short and humble experience rehabilitation for myocarditis and/or pericarditis should be a holistic approach. On one hand, like with any other injuries, you want to avoid stressing it while seeking out treatments that will put it on the right track that aids healing.
If you sprain your ankle, you can put your feet up, ice it a bit and rest it so it can heal. The heart has to work all the time so it is a trickier task to rest it completely as its function is involuntary under autonomic control.
In my experience, from advising my patients and seeing them benefit from other professional's advice, the below things tend to make a difference.
- Adjustment of nutritional habits - Embark on a so-called anti-inflammatory diet. This normally requires the elimination of foods and drinks that stress the body and fuels inflammation, like sugar and alcohol, trans fats... just to name the obvious, cutting out caffeine as in general we want the heart to rest, not to race and include nutrient dense anti-inflammatory foods full of anti-oxidants etc.
- Belonging to this category a whole list of nutritional supplements (that I won't detail such as quercetin, zinc, melatonin etc.) that seem to be helpful both to aid symptomatic management as well as to give your body the nutrients it needs to better manage inflammation. I would recommend seeing a nutritional therapist who has experience in advising on that also because you want to make sure that what you're taking is a) tailored to your body's needs and b) it works well with the medication you're taking, and not interacting with them.
- Hyperbaric Oxygen Therapy - without going into too much details, for this to be optimal you want to seek out a facility that has a hard shell capsule that provides 1.5 - 2 bar pressure. This, of course, should be supervised.
- Ozone blood treatment
- Cryotherapy/cold water exposure
I should also emphasise that the above should be done with the knowledge of your doctor/cardiologist who's probably already prescribed the necessary medications to both calm the inflammation and regulate your heart.
- Adjustments in in lifestyle and work-rest ratios which includes learning to know when to stop and rest to avoid being drained, which can cause a serious setback in your recovery.
- Meditation seems to be very useful especially for those who have a heard time relaxing and switching off.
- Manual & Exercise therapy
The goal of manual and exercise therapy
The physical rehabilitation side of things can be divided into two parts.
Targeted hands-on manual therapy to address the heart
Targeted exercise therapy to support the results of the manual therapy treatment
Low intensity steady-state cardiovascular exercise to build aerobic fitness in a targeted HR zone. This has to be slow and gradual and adopted based on your body's response. This is a tricky part as you need to increase the time spent doing physical activity in the required HR zone but it won't feel comfortable and you will need to push yourself but knowing when to push yourself and how much you should push yourself is the key to success because if you overshoot that can cause a flare up which can set you back significantly. This is much harder to learn for those who are used to exercising as the body responds differently to exercising than usual.
It is important to note that there is no one size fits all approach. What worked for others should be a guidance but it doesn't mean that it will work the same way for you.
You do need to seek out a professional that has experience with post-viral myo- or pericarditis. The same diagnosis can have different symptomatic representations and should be considered with what else might be going on in your body, so the approach should be tuned specifically to your body.
Inflammatory changes in the tissue can start a viscous cycle where movement feels uncomfortable and painful. The inflamed tissue is sensitive to tension and pressure.
In the case of the heart which sits between the two lungs on top of your main respiratory muscle the thoracic diaphragm, it is constantly under pressure and tension.
Once taking a deep breath becomes painful we tend to avoid it and start breathing more shallow.
Imagine going for a walk wearing a pair of shoes that just about fit your feet but as your feet swell during the walk your toes don't have enough space and starting to hurt.

When you breathe your respiratory muscles such as your diaphragm and intercostal muscles etc. contract which results in movement of your ribs, pulling on the pericardium, while there is an increased pressure in your thorax and abdomen with an expansion in the diameter of your ribcage and abdomen.

This movement of expansion is authorised by numerous small joints/articulations and many layers of connective tissue with liquid in between acting as a lubricant just like in a well-oiled engine. This movement is necessary and also serves to pump the liquid which in exchange ensures normal mobility of the adjacent layers on one another.
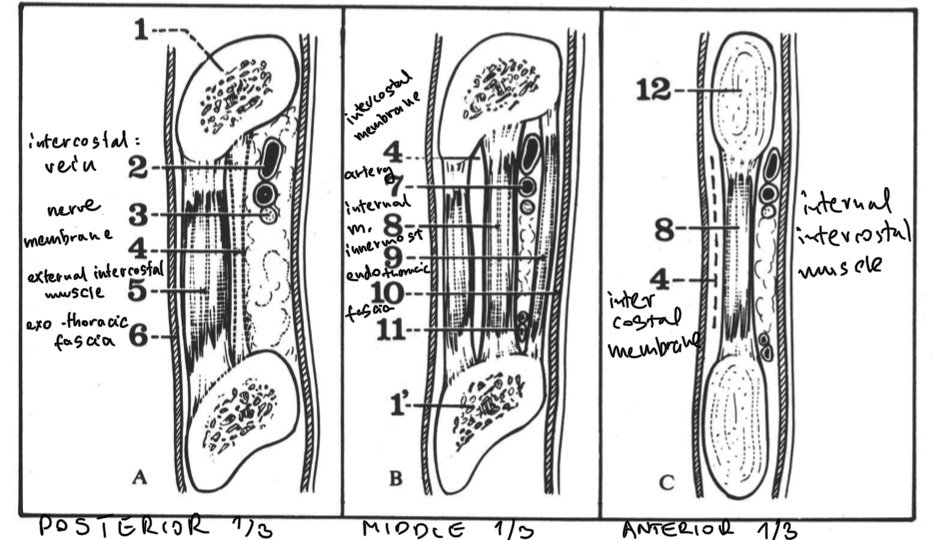
This illustration shows the different layers of muscles and connective tissues between the exothoracic fascia (which is the layer of connective tissue external and superficial to the ribs and intercostal spaces) and the endothoracic fascia (which is the connective tissue between the inside of the chest wall and the parietal layer of the plura of the lungs). There are as many as 7+layers that need to slide against on another. A good example of lack of movement can often be seen with the elderly and frail that bigger movement of a stiff spine and ribcage will elicit a coughing.
If these layers don't move well relative to one another, the viscosity of this liquid between layers of muscles and connective tissue changes to become more sticky and fails to fulfil its purpose as a lubricant. This will result in limitation of the thoracic cage/ribs to expand which also depends on the individual movements of the 12 pairs of costovertebral and costo-transverse joints of the ribs on the spine as well as the articulations of the ribs in the front with your sternum.

The pericardium is "suspended/attached to" the thoracic diaphragm, xiphoid and manubrium of the sternum, the cervical spine with links to the thyroid gland, oesophagus just to name a few.
Inferiorly the pericardium is sitting on the dome of the thoracic diaphragm and is attached to it by the phreno-pericardic ligament. Anteriorly the xypho-pericardic ligament. superiorly the vertebro-pericardic ligament to C6-7/T1 the manubrio-pericardic ligament and various fascial bands connecting to the thyroid cartilage the oesophagus etc. So just taking these few fascial links it is safe to say that the way you breathe and the way your diaphragm contracts and relaxes, the mobility of your ribcage as a whole as well as individual rib movements and the posture of your neck all have a direct impact on how the heart functions.
nflammation in certain cases can scar the muscle of the heart. Scaring can permanently change the affected tissue's ability to function normally. As a result the rest of the heart has to work harder to supply blood and oxygen around the body.
One of the main intention of targeted manual therapy in the treatment of pericarditis and myocarditis is to prevent the process of scaring by targeting the intrinsic mobility of the links of the heart and the spaces and structures around the heart via the movement of the ribs, the spine, the diaphragm, the oesophagus, trachea etc. By this we aim to improve the immediate environment of the heart to create a better environment for the tissue to function and heal.
Movement is life. Correct physiologic movement provides the right direction in the tension necessary to encourage and guide the body in the formation of new tissue.
The treatment plan works on different levels and stages:
As structure governs function we want to establish the normal mobility of joints and normalise key myofascial links.
Address the fascial/connective tissue links to the pericardium.
We want to work on the fibrous/parietal layer of the pericardium before addressing the serous or visceral layer in conjunction with the ANS (autonomic nervous system).
What can you expect from these treatments? While the end results depend on several different factors, patients can expect a significant reduction in the severity of their symptoms, the very least. The ultimate goal is to make it easier for the heart to heal, which means, continuous lessening of the severity of the symptoms, resolution of the inflamed cardiac tissue without fibrosis and scarring along with the recovery of normal ventricular function.
Disclaimer. This blog article is not meant to diagnose, treat or give any medical advice. This article only shares my views based on my experience working with patients who had these heart problems. You need to seek professional medical advice from your doctor if you experience heart problems.